
Diagnosing Food Allergy In Children
- Food allergy diagnoses are made based on more than just a simple lab test. Ordering testing for food allergy without supportive clinical history can lead to negative outcomes from ensuing misinterpretation and confusion. There are several factors that play a part in making the diagnosis of a true food allergy including: Patient symptoms, history of other allergic conditions, physical exam, skin prick test, IgE blood test, oral food challenge. There is a relatively high false positive rate with blood tests, which makes interpretation of the results dependent on clinical presentation as well.
- 90% of food allergies stem from: egg, wheat, milk, fish, shellfish, peanut, soy, and tree nuts.
Difference between Food Allergy vs Food Intolerance
- Food Intolerance refers to more common childhood symptoms or other unrelated chronic symptoms such as indigestion, abdominal pain or bloating, reflux, changes in bowel patterns and rashes
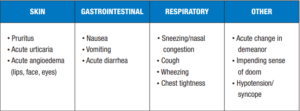
- IgE-mediated Food Allergy involves rapid reaction (within 1-2min) to specific foods with every ingestion and most commonly involves the following organ systems:
- Non-IgE- mediated Food Allergy: delayed onset allergic reaction (hours or days) that triggers a different mechanism of your immune system and most commonly involves the Gastrointestinal tract. These types of reactions are much more difficult to identity that cannot be detected with blood test and typically include food trials to identify.
- In the next posting we will discuss milk protein allergy which research is showing to become more and more prevalent.
Recommendations for decreasing the risk for food allergies
First: discuss with your provider to see if your baby is developmentally ready to consume complementary/table foods
- Introduce a variety of foods starting around 6 months. We usually recommend one new food every 3-4 days.
- Start with more typical table foods such as cereals, fruits and vegetables then if those are tolerated well, you may take the next step to introducing the foods more commonly linked to food allergy.
- Introducing peanut/tree nut products, egg or seafood: try for the first time at home with an anti-histamine on hand such as benadryl, rather than at a restaurant or daycare
- Don’t wait longer than 6-7mo to introduce high risk food products.
- For high risk patients, discuss with your provider introducing certain foods as early as 4mo. In some cases such as with children with severe eczema or a history of an immediate reaction while breastfeeding, an allergy evaluation or testing may be warranted before the introduction of certain foods.
When to be concerned!
- Signs of anaphylaxis include: shortness of breath, trouble breathing, swelling of lips or mouth, hives, vomiting, wheezing
- If patients has any of these symptoms give Benadryl and call 911 or go to the ER.
References:
- Nationwide Children’s. (2020). diagnosing food allergy in children. Diagnosing Food Allergy in Children, 1–4.
- Marill, M. C. (2021). Milk is overtaking nuts as top food allergy threat. Pediatric News, 55(6), 8.
- UpToDate. (n.d.). https://www.uptodate.com/contents/introducing-highly-allergenic-foods-to-infants-and-children?search=introducing+food&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2.

